Ivy @Ivy_4MJ 14m
Toxicologist Dan Anderson is on the stand at KJ- AEG trial. Here's a refresher of his testimony from Murray trial -
http://www.mjjcommunity.com/forum/threads/129310-Jacksons-vs-AEG-Day-5-May-6-2013-Discussion?p=3818662&viewfull=1#post3818662 …
8:49 PM - 6 Mai 13
Dan Anderson - Toxicologist on the stand,
Refresher: Dan Anderson testimony from Murray criminal trial Dan Anderson Testimony

Walgren directAnderson is employed by LA Coroner as a toxiologists for 21 years. His current position is the supervisor. He's responsible for the people and the results. Anderson mentions his education, work history and certifications.
Anderson talks in detail about toxicology, the type of tests they do ,the terms used and how they do the tests and the equipment they use.
Walgren starts talking about this case. Anderson received 4 samples of blood taken at the hospital and hand delivered to him by Fleak.
June 26. Anderson attended to the beginning of autopsy to tell what he wanted as samples. June 26 afternoon they started testing. Tests take several hour and days. They started evaluating them by Monday. They generated a 8 page report about all the samples tested.
ng/ml - nanogram ug/ml - micrograms. micrograms are 1000 times bigger than nanograms.
lunch breakMurray Trial Day 8 October 6, 2011
Afternoon session
Dan Anderson testimony continued
Walgren direct continuedAnderson goes over each of the findings in the report. Most majority of the test is done is using heart blood. It's the starting point.
-Femoral blood is taken from leg.
-Heart blood is taken from heart.
- Hospital blood is taken at hospital.
- Vitreous fluid is taken from behind the eyeballs.
- Liver they took a portion.
- Gastric contents are stomach contents.
- Urine samples : Urine from scene brought in a plastic urine bottle also they collected urine from the bladder during autopsy
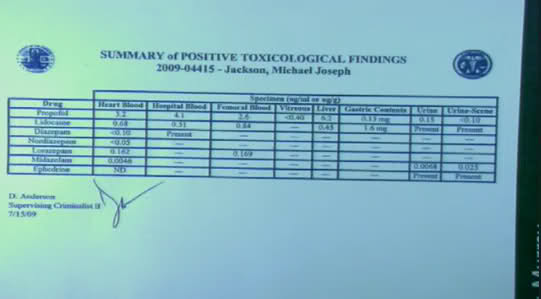
Anderson lists all the findings. You can see some of them in the following pictures. For full details check the the autopsy report.
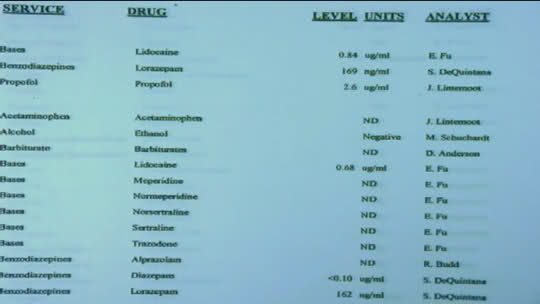
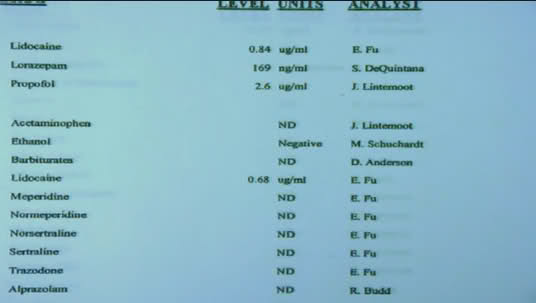
Important findings: MJ had no alcohol, no Demerol (Meperadine) , no metabolized Demerol (normeperidine) and no Cocaine, Marijuana and such. MJ had Valium, Lorezepam and Midazolam, Propofol in his system. They tested femerol blood, heart blood and hospital blood. They did 2 tests on liver for lidocaine and propofol - both was detected in liver. Stomach contents showed Lidocaine and Propofol. Urine from autopsy shows lidocaine, Midazolam, Ephedrine and Propofol. Jug of urine was tested and it showed Lidocaine, Midazolam, Ephedrine and Propofol. Vitreous (clear fluid behind the eye) showed Propofol.
Anderson made a summary about positive toxicology findings.

Walgren again clearly states that there was no Demerol in MJ's system. Anderson says correct.
Walgren mentions Propofol in MJ's stomach. Anderson compares amount of propofol in MJ's stomach is equivalent to 'specks of sugar granules'. So they are basically saying that it's too small.
Syringe on the nightstand was tested. They found 4 drops of liquid in it. They detected propofol and lidocaine in it.
Saline bag, tubing, Y connector and syringe on the IV was tested. They draw a diagram and determined how to test it. Walgren identifies each of the items.
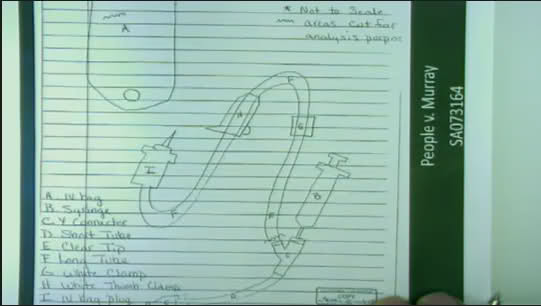
Propofol, lidocaine and flumazenil was found on the IV on the syringe and the short side of the tubing. Saline bag and long section of IV tubing had no drugs detected.

mid afternoon break.
Flanagan CrossFlanagan is going over the summary report about positive toxicology findings.
Flanagan asks why Propofol was tested on 3 different blood samples. Anderson says they generally make tests on 2 samples : general blood and peripheral blood (such as from the leg femoral blood) due to postportem distribution. Anderson explains that the body tissue releases the drugs back into the circulation after death and moving the body will also distribute the drugs. On this instance they also got hospital admittance blood.
Flanagan asks if the reason for hospital blood result be higher is due to the drugs not having chance to be redistributed. Objection. Judge finds the question vague. Flanagan " Do you know why the hospital blood results are higher?" Answer : No. Flanagan "why is the femoral blood results are the lowest?" Answer : Postportem distribution. Flanagan confuses the witness to the point that he can't understand what is being asked. Flanagan "Why is femoral blood has the lowest results?" Answer : That's typical because tissues release drugs to the central cavity artifically raising the heart blood.
Lidocaine higher in femoral blood then the heart blood. Anderson says it's drug dependent. Some drugs might have different distribution pattern.
Flanagan asks why the eye fluid was analyzed. They analyzed it for Propofol because Propofol was the real issue. Anderson says that they didn't have enough fluid to make a full analysis. It tells him that Propofol doesn't distrubute very well to the eyeball fluid. They didn't give an exact number amount for Propofol in the eye fluid because they didn't have enough sample. Protocol tells that they can't give exact numbers in such instances as they can't gurantee the accuracy.
Urine from the scene. Flanagan asks why they couldn't get the exact number amount for Propofol amount. Again It was below their lowest caliber. It was almost negligible.
Ephedrine was present in the urine but wasn't in blood. It's because bladder can store things for a long time. Flanaggan asks how long ago it was used. Anderson says it can't be recent as it's not in the blood and it could be used anywhere between 24 to 72 hours ago.
Propofol was found in the urine from the scene. Flanagan asks if it could be from a few days ago as well. Anderson agrees and says that it could also be recent. Flanagan asks if the urine from the scene was accumulated before urine from autopsy. Anderson says he has no idea when it was collected or even it's from MJ.
Flanagan gives a scenario that the urine from the scene was in 7 AM and the time of death being around 12:00 and 2:26 and says that not much urine is collected after death. Anderson corrects him that they actually had over 500 ml of autopsy urine which he says to be alot.
Flanagan is trying to say that MJ got/given propofol after the urine in the scene was deposited in the plastic bottle because the propofol level was higher in the autopsy urine. Flanagan again confuses the witness and no one can understand what he's asking.
Lorazepam. Flanagan asks if it's high. Anderson says it's normal high therapeutic range. Flanagan asks how much lorazepam MJ was given in mg. Anderson says that calculation could be done but it would not be a perfect calculation as there has to be several assumptions made. Anderson says it shouldn't be done.
Anderson mentions assumptions that needed for such calculation :drug fully distributed, redistrubution didn't happen after death and the heart blood level is not falsely elevated.
Flanagan shows a book saying that Lorazepam is not subject to redistribution after death. Anderson doesn't agree with it and says there have been only 2 cases stating that but he wouldn't be comfortable with generalizating it to the whole population.
Flanagan still asks Anderson to give a mg number. Anderson goes over his records saying that based on several assumptions, it's approximately 11 mg. Anderson says that they can't determine how Lorazepam was given (orally or IV) from a blood level and he doesn't know when it was given.
Flanagan asks if the results indicate that lorazepam has been in the system for a while. Anderson says yes. Propofol levels was not equilibrium. Flanagan asks if a person was on a drip , would he expect the propofol levels to be in equilibrium. Anderson says he doesn't know how Propofol metabolizes.
Flanagan mentions that the summary Anderson did has no information about Lorazepam in the stomach contents. Anderson says that they only analyze stomach contents for overdose cases. Their blood test results showed Lorazepam to be in the acceptable range so they didn't test it in the stomach.
Defense has tested the stomach for Lorazepam , it was .634 micrograms/ml.
Flanagan says Lorazepam is 4 times concentrated in the stomach then the blood. Anderson disagrees saying that it's not significant in it's opinion. Flanagan asks if it's consistent with oral digestion. Anderson says no and explains that drugs will be in stomach in small levels due to "ion trapping" and doesn't necessarily mean that it's taken orally. Anderson converts it to mg : 0.046 mg , that means 1/40th of a normal 2 mg pill. Anderson says that it could come from the blood.
Flanagan asks questions about Midazolam. Anderson has not made calculations about it because the amounts are really small.
Flanagan by looking to urine level of Midazolam trying to establish blood levels for it. Anderson says it's not a comparison that could be done.
Flanagan talks about urine and whether it would be representative of the metabolization of the drugs such as if a person urinated at 1 AM and then at 7 AM , Flanagan asks if the 7 AM urine would be representative of the 1 AM - 7AM period. Anderson says there will be some contamination. Flanagan asks if the autopsy urine would be an average level of 12:30 - 7:30 AM time period. Anderson is having trouble with understanding the question. Judge and Walgren also doesn't understand the questions. Flanagan asks if urine would be in equilibrium with the blood, it's beyond Anderson's level of expertise. Anderson says just from the urine results he cannot tell when the person would have higher levels of Midazolam in his system. Anderson says he can't do it for Propofol as well.
Back to stomach contents and not analyzing it for Midazolam and Lorazepam. Switching to IV set testing. Saline bag and the tubing that goes down to the y port had no propofol or lidocaine. Propofol, lidocaine and flumazenil was found in the syringe and short tubing. Flanagan asks about the amounts of those drugs. Anderson says that they didn't quantify them because they didn't think it was relevant and they didn't have a standard procedure to quantify fluids from medical evidence. Flanagan asks if they can tell the proportions of lidocaine and propofol and flumazenil. Anderson says they can't. Anderson says they also had a very small amounts of liquids that complicated the testing as well.
end of day 8Murray Trial Day 9, October 7, 2011
Morning Session
Dan Anderson Testimony continuedFlanagan Cross continued
Flanagan starts off by asking about the IV bag on the stand in MJ's room where he died. Flanagan asks if the bag was analyzed for all chemicals and the only thing was saline solution, Anderson states they do not analyze for solution, but there were no drugs found in it. Flanagan asks about the tubing (hanging from the IV stand), and Anderson states that it was not found to have any drugs in it.
Flanagan asks repeatedly whether the tubing and the IV bag were attached, Anderson repeatedly states that they were not attached when received into medical evidence, according to notes. Flanagan asks if Anderson tested two syringe barrels, Anderson states yes and when asked, states that both barrels tested positive for propofol and lidocaine. Flanagan asks if Anderson tested any apparatus that had only propofol in it, Anderson states no. Anderson states that the only medical equipment that had propofol and lidocaine in them were the Y tubing (connector) and the syringe barrels. Anderson states that each of the syringes and the Y tubing each had Flumanezil. Flanagan asks if the proportion of propofol and lidocaine were the same in both the Y tubing and the 2 syringe barrels, Anderson states that proportionality testing was not performed.
Flanagan asks for Anderson to define equilibrium as it relates to bodily fluids, Anderson states he believes it is when the samples of the drug or their concentrations are equal. Flanagan asks how long it takes for the blood system to come to an equilibrium, Anderson states its beyond his scope of expertise. Flanagan asks Anderson to define therapeutic range (of a drug), Anderson states that a concentration of the drug that achieves the desired effect, generally it is a safety concern because they are not safe at all concentrations. Flanagan asks what determines therapeutic range, Anderson states clinical trials from the FDA, as well as the literature provided with each drug. Flanagan asks if there is a therapeutic range for propofol, Anderson states no. Flanagan asks about therapeutic range for Lorazepam, Anderson states that it averages 100-200 micrograms per mililiter. Anderson clarifies that the average can be 180, but that everybody tolerates medications differently, and he cannot give specific ranges.
Flanagan shows a Lorazepam bottle, prescription for MJ, asks Anderson to read the bottle, Anderson reads Lorazepam 2 mgs, 1 tablet by mouth. Flanagan asks about MJ's blood concentration of .16% and asks if that would equal about five Lorazepam tablets, Anderson states yes, regardless of the route, whether it was in tablet or IV form. Flanagan asks if MJ had the equivalent of 11 mg of Lorazepam, Anderson states yes, approximately. Flanagan asks how many pills would MJ have to take to get to that level (11 mg), Anderson states that it could be an accumulation over several days, and that he does not feel comfortable with assumptions of routing of medications or form of medications.
Flanagan asks about ion trapping with respect Lorazepam, Anderson states that he knows little about Lorazepam and postmortem redistribution. Anderson states that the only way to get propofol in the stomach is through oral ingestion or ion trapping, it's not postmortem redistribution.
Flanagan asks Anderson to define the term ion trapping. Anderson states that an acidic environment traps the ions of the drug in that environment, beyond that, is beyond his area of expertise. Anderson states that other than ingestion, the only way propofol can get into the stomach by diffusion of the surrounding specimens. When Flanagan asks about the surrounding specimens, Anderson answers that the liver is close, blood samples and blood itself are close to the stomach.
Flanagan states that Anderson is saying that Lorazepam can get into the stomach through redistribution, Anderson states that it can get into the stomach by ion trapping. Anderson states time and time again that this information is beyond the scope of his expertise. Anderson states that he has seen many different decendents who had stomach contents with drugs in them, and that the drugs were not given orally.
Anderson states he does not have personal experience with a decendent that had Lorazepam in their stomach.
Flanagan asks Anderson about ephedrine. Flanagan asks if Anderson came to understand that propofol was the most important drug in the case, Anderson states yes he did. Flanagan asks if Lorazepam was important, Anderson he thinks it has its importance, but that it does notraise a flag. Anderson states that propofol in any case is important, Lorazepam was in therapeutic range, and that he previously testified that propofol was within range only a proper setting. When Flanagan asks what does a setting have to do with therapeutic range, Anderson states that it's very important. Flanagan states that therapeutic range is desired effect, Anderson states yes. Flanagan states that the literature does not take into consideration the setting, Anderson states that every drug literature takes setting into consideration.
Flanagan asks if Anderson did the calculations with regard to Lorazepam last weekend, Anderson states it was two weekends ago, Anderson states that he did them because of the Lorazepam in the gastric sample, and the two urine samples done by the defense. Anderson states that the urine is a historical perspective, and could be an accumulation from several days. Anderson states that the Midazolam testing was done in the urine because the concentration is much higher, which helps to confirm the blood level of Midazolam. Anderson states that Lorazepam levels were much more elevated in the urine than the Midazolam. Anderson states Lorazepam 12,974 nanograms/ml (13 micrograms/ml) Midazolam 0.025 nanograms/ml. Anderson states that the Lorazepam concentration goes up in the autopsy urine, and with Midzolam much less than Lorazepam.
Anderson states that the half life of Lorazepam is 9-16 hours, and that he looked it up in a medical reference book to gain that information. Anderson states he doesn't know what the absorption time and/or the peak time of Lorazepam, that it is in the book, but he doesn't remember what it said.
Walgren RedirectAnderson clarifies that he never went to 100 North Carolwood. Anderson states that he received vials of blood, a broken syringe with plunger, an IV catheter from Investigator Fleak. Anderson states that the IV bag and IV tubing was brought to him at the lab, simply marked medical evidence #2.
Anderson states that the difference between blood sample and urine sample, is that the blood is what is usually happening in the body, and in the urine represents everything that the body is metabolizing out, and that the urine concentration expectation is that it would be much higher. Anderson states that the urine is historical in nature and what is being expelled from the body over a certain amount of time.
Anderson states that the PACTOX gastric contents analysis, shows 634 nanograms/ml of Lorazepam. Anderson states that the lab measured in concentration, he was provided 73.5 mls of gastric contents, in which he would multiply the two numbers to get the nanograms of stomach contents which would be 46,599 nanograms of Lorazepam left in the stomach. But the numbers Anderson should have used for calculation (micrograms not nanograms) he needed to divide by a thousand, so 46,599 divided by a thousand equals 46.599 divided by another 1000 to get a mg amount, equals 0.04599 of Lorazepam in the stomach. Anderson states that he went further and got a more exact amount and arrived at 0.046599. Anderson states that with a 2 mg Lorazepam pill, the gastric contents are equal to 1/43rd of a single 2 mg tablet, which is a very small amount
Flanagan RecrossFlanagan asks if there is a high concentration of ephedrine in the urine, but a low concentration in the bladder, would it be fair to say it was recently taken, Anderson says it’s a fair assumption. Flanagan asks if it's the same with propofol, Anderson states that he is not familiar with the excretion patterns of propofol.
Flanagan asks if a person were to take 7 or 8 Lorazepam tablets, and he found 14 miligrams in the stomach, would Anderson state that the person had taken it recently, Anderson states yes. There are numerous questions asked after this by Flanagan, but prosecutor Walgren objects and judge Pastor sustains them.